第五届中国出版政府奖音像电子网络出版物奖提名奖
中国科技核心期刊
中国科学引文数据库(CSCD)来源期刊

第五届中国出版政府奖音像电子网络出版物奖提名奖
中国科技核心期刊
中国科学引文数据库(CSCD)来源期刊
2022 , Vol. 08 >Issue 02: 121 - 125
DOI: https://doi.org/10.3877/cma.j.issn.2096-1537.2022.02.007
不同头高位对aSAH患者术后颅内压及脑灌注压的影响
Copy editor: 卫轲
收稿日期: 2022-04-07
网络出版日期: 2022-07-05
基金资助
首都医科大学附属北京天坛医院人才引进项目(2-1-1-469-01)
版权
Effects of different head heights on intracranial pressure and cerebral perfusion pressure in postoperative aneurysmal subarachnoid hemorrhage patients
Received date: 2022-04-07
Online published: 2022-07-05
Copyright
探讨不同头高位对动脉瘤性蛛网膜下腔出血(aSAH)患者术后颅内压和脑灌注压的影响。
纳入66例2020年9月至2021年4月我院重症医学科aSAH术后患者,依次将床头抬高0°、10°、20°、30°、40°,每种体位保持15 min,待稳定后记录患者血压、心率、呼吸、脉搏血氧饱和度、颅内压,计算出相应平均动脉压和脑灌注压。并收集患者的预后相关指标,包括压力性损伤、住院病死率、出院时格拉斯哥预后评分。
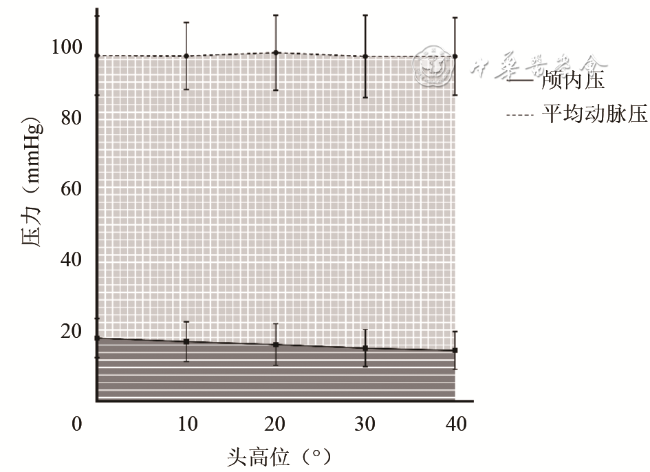
在床头抬高0°、10°、20°、30°、40°时,颅内压分别为(17.76±5.54)、(16.77±5.58)、(15.94±5.85)、(14.94±5.26)、(14.35±5.33)mmHg(1 mmHg=0.133 kPa),脑灌注压分别为(79.31±12.08)、(80.17±10.07)、(81.94±11.96)、(81.92±12.48)、(82.53±12.30)mmHg,平均动脉压分别为(97.07±11.17)、(96.94±9.43)、(97.88±10.57)、(96.86±11.56)、(96.87±10.89)mmHg。头高位从0°增加到30°时,颅内压显著下降,差异有统计学意义(两两比较,P=0.001,P=0.050,P=0.033),但在30°与40°时,差异无统计学意义(P=0.507)。头高位从0°增加到40°时,脑灌注压呈升高趋势,差异有统计学意义(P=0.031),但两两比较,差异无统计学意义(均P>0.05)。平均动脉压随着头高位角度的增高并没有明显变化,差异无统计学意义(P=0.826)。患者在不同头高位下的收缩压、舒张压、心率、呼吸、脉搏血氧饱和度等生命体征比较,差异均无统计学意义(均P>0.05)。所有患者ICU住院期间均未发生压力性损伤。
对aSAH术后患者,床头抬高至30°~40°是控制颅内压升高、保证有效脑灌注压的安全有效的治疗性体位。对初始颅内压较高的患者,床头抬高至40°可降低颅内压,且无需担心压力性损伤的发生。
关键词: 动脉瘤性蛛网膜下腔出血; 头高位; 颅内压; 脑灌注压
曹炜 , 王翠雪 , 徐珊珊 , 袁媛 , 张琳琳 , 周建新 . 不同头高位对aSAH患者术后颅内压及脑灌注压的影响[J]. 中华重症医学电子杂志, 2022 , 08(02) : 121 -125 . DOI: 10.3877/cma.j.issn.2096-1537.2022.02.007
To investigate the effects of different bedside angle on postoperative intracranial pressure and cerebral perfusion pressure in aSAH patients.
66 postoperative aSAH patients in the intensive care unit of Beijing Tiantan Hospital, Capital Medical University from September 2020 to April 2021 were selected as the research objects. The patients in a supine position at rest and raise the bedside angle by 0°, 10°, 20°, 30° and 40°) were kept in turn. Each position was held for 15 minutes, in which blood pressure, heart rate, respiration rate, pulse oxygen saturation and intracranial pressure were recorded after the data was stable. The average arterial pressure and cerebral perfusion pressure were calculated correspondingly. Prognostic related parameters including pressure injuries, hospital mortality, and Glasgow score at discharge, were also collected.
When the bedside angle were elevated at 0°, 10°, 20°, 30° and 40°, the intracranial pressure values were (17.76±5.54), (16.77±5.58), (15.94±5.85), (14.94±5.26), (14.35±5.33) mmHg (1 mmHg=0.133 kPa); the cerebral perfusion pressure were (79.31±12.08), (80.17±10.07), (81.94±11.96), (81.92±12.48), (82.53±12.30) mmHg, and the mean arterial pressure were (97.07±11.17), (96.94±9.43), (97.88±10.57), (96.86±11.56), (96.87±10.89) mmHg, respectively. The intracranial pressure decreased significantly with the increase of bedside angle from 0° to 30° (pairwise comparison showed P=0.001, P=0.050 and P=0.033), there was no significant difference in intracranial pressure between 30° and 40° (P=0.507). The cerebral perfusion pressure had a growing trend with the increase of the bedside angle from 0 ° to 40° (P=0.031), but there was no significant difference in all of pairwise comparison (P>0.05). Mean arterial pressure did not change significantly with the increase of the degree of head elevation (P>0.05). There was no statistically significant difference in vital signs of systolic blood pressure, diastolic blood pressure, heart rate, respiration rate and pulse oxygen saturation at different degrees of head elevations (P>0.05). No pressure injury occurred in all patients during their ICU stay.
It may be a safe and effective therapeutic position to maintain the bedside angle at 30°-40° in aSAH patients to control intracranial pressure and ensure adequate cerebral perfusion. For patients with initially high intracranial pressure, raising the bedside angle to 40° may reduce intracranial pressure without increasing risks of pressure injuries.
表1 不同头高位对aSAH术后患者脑血流动力学的影响(mmHg, |
| 头高位 | 颅内压 | 平均动脉压 | 脑灌注压 |
|---|---|---|---|
| 0。 | 17.76±5.54 | 97.07±11.17 | 79.31±12.08 |
| 10。 | 16.77±5.58 | 96.94±9.43 | 80.17±10.07 |
| 20。 | 15.94±5.85 | 97.88±10.57 | 81.94±11.96 |
| 30。 | 14.94±5.26 | 96.86±11.56 | 81.92±12.48 |
| 40。 | 14.35±5.33 | 96.87±10.89 | 82.53±12.30 |
| F值 | 27.485 | 0.343 | 2.925 |
| P值 | <0.001 | 0.826 | 0.031 |
注:aSAH为动脉瘤性蛛网膜下腔出血;1 mmHg=0.133 kPa |
表2 头高位逐渐增加时aSAH术后患者颅内压、脑灌注压的变化(mmHg, |
| 头高位变化 | 颅内压平均值差值* | P值 | 脑灌注压平均值差值* | P值 |
|---|---|---|---|---|
| 0。到10。 | 0.99±0.24 | 0.001 | -0.86±0.93 | 0.999 |
| 10。到20。 | 0.83±0.29 | 0.050 | -1.77±1.01 | 0.849 |
| 20。到30。 | 1.00±0.33 | 0.033 | 0.02±1.19 | 0.999 |
| 30。到40。 | 0.59±0.30 | 0.507 | -0.61±0.99 | 0.999 |
注:*差值为头高位较低时的数值减去头高位较高时的数值;aSAH为动脉瘤性蛛网膜下腔出血;1 mmHg=0.133 kPa |
表3 不同头高位对aSAH术后患者生命体征的影响( |
| 头高位 | 收缩压(mmHg) | 舒张压(mmHg) | 心率(次/min) | 呼吸(次/min) | 脉搏血氧饱和度 |
|---|---|---|---|---|---|
| 0。 | 136.07±15.47 | 79.34±13.52 | 84.10±15.80 | 17.77±4.49 | 0.984±0.270 |
| 10。 | 136.71±16.01 | 78.59±10.89 | 82.81±14.21 | 17.77±4.43 | 0.990±0.165 |
| 20。 | 137.50±16.91 | 80.10±11.58 | 83.11±14.50 | 17.46±4.13 | 0.973±0.108 |
| 30。 | 136.41±15.05 | 78.06±13.85 | 83.54±16.75 | 17.04±3.93 | 0.986±0.015 |
| 40。 | 135.73±15.13 | 78.60±12.00 | 83.47±15.27 | 18.50±9.17 | 0.986±0.016 |
| F值 | 0.130 | 0.287 | 0.070 | 0.614 | 0.392 |
| P值 | 0.972 | 0.886 | 0.991 | 0.653 | 0.815 |
注:aSAH为动脉瘤性蛛网膜下腔出血;1 mmHg=0.133 kPa |
| 1 |
国家神经系统疾病医疗质量控制中心. 2020年国家医疗服务与质量安全报告——神经系统疾病分册 [M]. 北京: 人民卫生出版社, 2021: 131-140.
|
| 2 |
|
| 3 |
|
| 4 |
典慧娟, 范艳竹, 王琳琳, 等. 体位及头高位对重型颅脑损伤病人颅内压和脑灌注压的影响 [J]. 护理研究, 2020, 34(14): 2520-2523.
|
| 5 |
|
| 6 |
|
| 7 |
孙红. 北京协和医院重症医学科护理工作指南 [M]. 北京: 人民卫生出版社, 2016: 160-163.
|
| 8 |
江燕, 袁萍, 张燕茹, 等. 脑出血患者静息状态下不同头位抬高角度对颅内压和脑血流量的影响 [J]. 中国实用护理杂志, 2020, 36(22): 1700-1704.
|
| 9 |
鲁林, 戴新娟, 杨敏. 不同角度头高位对重型颅脑损伤患者颅内压及脑灌注压的影响 [J]. 中国实用护理杂志, 2016, 32(35): 2742-2745.
|
| 10 |
|
| 11 |
刘义兰, 段征征, 邓先锋, 等. 湖北省住院患者压疮现患率的调查研究 [J]. 中国护理管理, 2015, 15(2): 209-211.
|
| 12 |
|
| 13 |
冷玉鑫, 张楠, 朱曦, 等. 抬高体位对机械通气患者腹腔压力和胃食管反流的综合影响 [J]. 中国危重病急救医学, 2011, 23(9): 534-538.
|
| 14 |
肖春雪, 石建秋, 赵一雷. 不同体位对高血压脑出血病人颅内压、脑灌注压和生命体征的影响 [J]. 蚌埠医学院学报, 2017, 42(10): 1408-1410, 1414.
|
/
| 〈 |
|
〉 |


{kind=link}
{kind=link}