
对象与方法
一、文献检索
参照Cochrane协作网制定的检索策略进行检索,包括计算机检索和手工检索。
(一)计算机检索
检索PubMed、the Cochrane Library、Embase、Web of Science等数据库。检索时限为1970年1月1日至2020年12月31日。英文检索词及检索式为:“right heart” OR “right ventricular”,AND “extracorporeal membrane oxygenation” OR “ECMO” OR “Extracorporeal life support”。
(二)手工检索
将以上检索到的文章题目和作者等资料制表,筛选出重复文献;追查已纳入研究的参考文献。
二、文献纳入及排除标准
(一)纳入标准
(1)对照或非对照研究;(2)纳入病患有心功能不全(心脏衰竭),接受ECMO干预,并且心功能不全发生于ECMO干预之前;(3)所有研究必须提供以下至少1项研究终点:1个月病死率、住院病死率、3个月存活率、6个月存活率、1年存活率、住院存活率或总存活率。
(二)排除标准
(1)病例数<5例;(2)无量化数据的文献;(3)文献来源为个例报道、综述、会议报告。
三、数据提取及文献质量评价
本荟萃分析遵循系统综述与荟萃分析优先报告条目(PRISMA)规范。2名评价者独立进行文献检索、筛选文献、资料提取和质量评价,并交叉核对,确保一致。如有分歧,则通过双方讨论或第3名评价者协助解决。数据不全或者形式不同时,通过与作者联系予以补充,无法获得资料的文献则不处理。资料提取的内容包括:(1)纳入研究的基本信息,如研究题目、第一作者、发表杂志等;(2)研究对象的基线特征和附加的干预措施;(3)所关注的结果数据。
采用Newcastle-Ottawa scale(NOS)评分标准对所选的文献进行评估,该量表主要由3个因素组成:研究对象选择、研究组间可比性、结果评估。每个观察性研究0~10分,质量分数≥7分则定义为高质量研究。
四、统计学分析
统计分析采用2.0版本的Comprehensive Meta-Analysis statistical software,version(Biostat,Englewood,NJ,USA)。连续变量采用
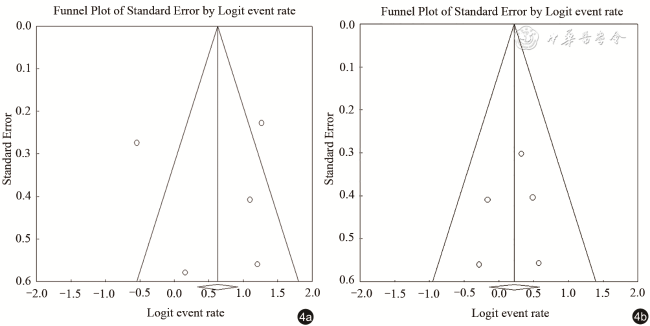
±s或M(Q25,Q75)表示,分类变量采用例(%)表示。将所有纳入研究的个别数值合并,得到一个总结估计值(summary effect),并计算其95%CI。通过同时计算Cochran Q和I2来评估不同篇研究数值间的异质性。I2表示异质性引起的研究值间变异性的百分比,进一步定义为0≤I2<25%表示无异质性,25%≤I2<50%为中度异质性,50%≤I2<75%为高度异质性,75%≤I2<100%则为极端异质性。如果研究之间存在异质性(I2>50%),则采用随机效应模型(DerSimonian-Laird方法),反之则采用固定效应模型(Mantel-Haenszel方法)。以均值变化合并差异,双侧P值<0.05为差异有统计学意义。采用省略法进行敏感度分析。当纳入5篇或5篇以上的研究进行荟萃分析时,采用漏斗图和单边Egger's检验评价呈现是否偏倚。

结果
一、文献检索结果及纳入文献基本信息
通过对所选数据库的检索,共检索出文献1048篇,按照纳入排除标准进行筛选,排除与主题无关文献987篇,缺少数据文献39篇,排除重复文献4篇,最终有18篇文献最终被纳入研究,共计729例患者(图1 )。729例接受ECMO干预的心脏衰竭患者中,185例有左心室辅助装置,69例同时有左心室加上右心室辅助装置,57例同时有左心室辅助装置与双心室辅助装置(BVAD),375例无辅助装置,43例数据缺失。每篇研究的患者总数为5~202例。纳入研究及患者基本信息见表1 。
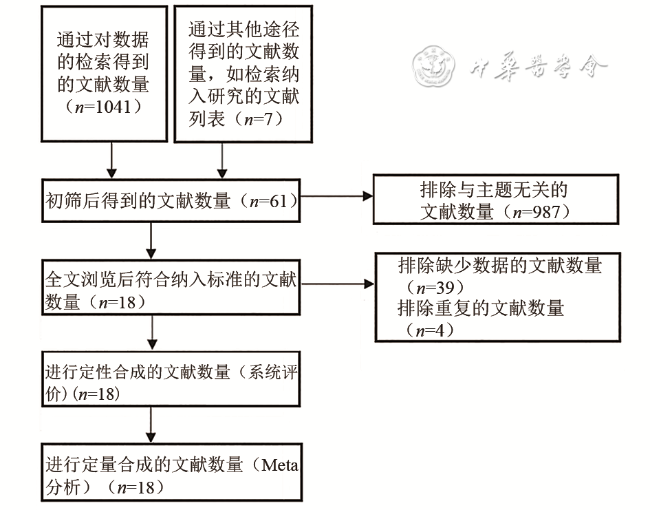
表1 纳入研究及患者的基本特征信息 |
| 研究者 | 年份 | 辅助装置 | 例数 | 年龄(岁) | 男性比例[例(%)] | 病死率 | 生存率 |
|---|---|---|---|---|---|---|---|
| Djordjevic,I | 2020 | 无 | 64 | 63±14 | 42(68) | 1个月病死率88% | - |
| Riebandt,J | 2018 | 左心室辅助 | 32 | 52±14 | 27(84.4) | 1个月病死率18.8%,住院病死率25% | 1年生存率75% |
| den Uil,CA | 2017 | - | 29 | 40±16 | 12(41) | 3个月病死率38% | 3个月生存率62% |
| Fischer,Q | 2018 | 左心室辅助+右心室辅助 | 44 | 58.2±12.3 | 38(86) | - | 1、3、6个月生存率 88.4%,78.2%,66.1% |
| Shehab,S | 2018 | 左心室辅助 | 112 | 51±14 | 90(80) | - | 1年生存率78% |
| Han,JJ | 2018 | 左心室辅助 | 18 | 54±16 | 14(78) | - | 1年生存率77% |
| Leidenfrost,J | 2016 | 左心室辅助+右心室辅助 | 12 | 45.6±16 | - | 1个月病死率8% | 3、6个月、1年生存率 86%,63% and 54% |
| Schoenrath,F | 2016 | 左心室辅助+双心室辅助 | 57 | 46.8±15.5 | 13(43.3) | - | 1、2、4年生存率6.8%,32.2% and 29.8% |
| Acheampong,B | 2016 | 无 | 24 | 41(22~75) | 14(58.3) | 住院病死率54% | 住院生存率 46% |
| Noly,PE | 2014 | 左心室辅助 | 8 | 50.8±9.9 | 5(62.5) | 病死率50.00% | - |
| Scherer,M | 2011 | 左心室辅助 | 10 | 53±10 | 9(90) | - | 总生存率60% |
| Chou,NK | 2010 | - | 14 | - | - | - | 总生存率69.2% |
| Bautista-Hernandez,V | 2009 | 无 | 26 | 0.12(0~193)* | 18(69) | - | 住院生存率62% |
| Luo,XJ | 2009 | 无 | 45 | 49.0±14.1 | 34(76) | 住院病死率42% | 住院生存率58% |
| Scherer,M | 2009 | 左心室辅助 | 5 | 47±11 | 4(80) | - | 总生存率80% |
| Liu,KS | 2009 | 无 | 14 | 55.7±15.4 | 7(50) | - | 住院生存率64% |
| Taghavi,S | 2004 | 左心室辅助+右心室辅助 | 13 | 51.3±15.6 | 10(77) | - | 住院生存率43% |
| Smedira,NG | 2001 | 无 | 202 | 55±14 | 145(72) | - | 1个月、1年生存率8%,24% |
注:“*”单位为个月;“-”代表无数据 |
二、文献质量评价
文献NOS量表评分显示,有8篇文献为6分,6篇文献为7分,4篇文献为8分(表2 )。
表2 文献NOS量表评分(分) |
| 研究者 | 年份 | 对象的选择 | 群体可比性 | 结局评估 | 合计 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1* | 2* | 3* | 4* | 5* | 6* | 7* | 8* | |||
| Djordjevic,I | 2020 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Riebandt,J | 2018 | 1 | 0 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| den Uil,CA | 2018 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 6 |
| Fischer,Q | 2018 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 6 |
| Shehab,S | 2018 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 6 |
| Han,JJ | 2018 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Leidenfrost,J | 2016 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 6 |
| Schoenrath,F | 2016 | 1 | 0 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Acheampong,B | 2016 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Noly,PE | 2014 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 6 |
| Scherer,M | 2011 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 6 |
| Chou,NK | 2010 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 6 |
| Bautista-Hernandez,V | 2009 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 6 |
| Luo,XJ | 2009 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Scherer,M | 2009 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Liu,KS | 2009 | 1 | 0 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Taghavi,S | 2004 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Smedira,NG | 2001 | 1 | 0 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
注:1*为暴露队列的代表性;2*为非暴露队列的选择;3*为暴露确认;4*为研究开始前没有研究对象发生结局事件;5*为基于设计或分析所得的队列的可比性;6*为结局事件的评估;7*为观察到结局发生,随访是否充分;8*为随访的完整性 |
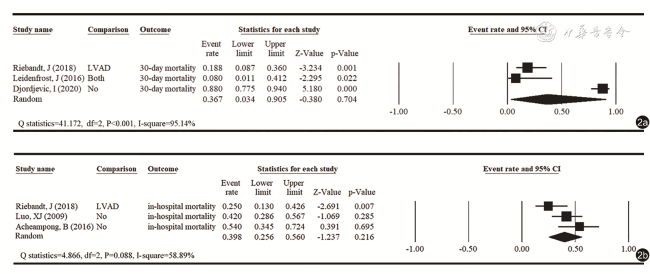
三、1个月病死率及住院病死率分析
18篇纳入文献中,有3项研究提供了关于1个月病死率的信息,异质性检验呈现高度异质性(I2=95.14%),荟萃分析结果显示,心功能不全患者通过ECMO干预,1个月病死率为36.7%(95%CI:0.034~0.905);4项研究提供了住院病死率的信息,异质性检验呈现高度异质性(I2=58.89%),荟萃分析结果显示,住院病死率为39.8%(95%CI:0.256~0.560)(图2 )。
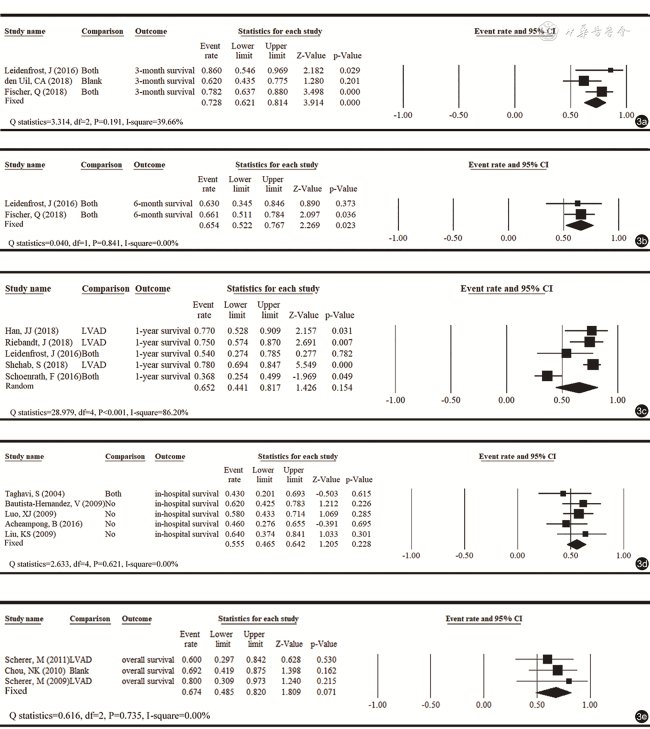
四、3个月、6个月、1年存活率,住院存活率及总存活率分析
18篇纳入文献中,有4篇研究提供了3个月存活率,2篇研究提供了6个月存活率,5篇研究提供了1年存活率,5篇研究提供了住院存活率,3篇研究提供了总存活率。1年存活率结局的异质性检验呈现高度异质性(I2=86.20%)。荟萃分析结果显示,心功能不全患者通过ECMO干预,3个月存活率为72.8%(95%CI:0.621~0.814),6个月存活率为65.4%(95%CI:0.522~0.767),1年存活率为65.2%(95%CI:0.441~0.817),住院存活率为55.5%(95%CI:0.465~0.642),总存活率为67.4%(95%CI:0.485~0.820)(图3 )。
五、敏感度分析
采用“leave-one-out”方法对纳入的临床文献结果进行敏感度分析,结果见表3 、4 。除去个别研究后,病死率和存活率的总结估计的方向和幅度均没有显著变化,这表明对这些纳入文献的荟萃分析结果不受个别研究过度影响。
表3 病死率的敏感度分析 |
| 结果 | 文献 | 统计结果 | ||
|---|---|---|---|---|
| 分数 | 95%CI | P值 | ||
| 1个月病死率 | Riebandt,J(2018) | 0.472 | 0.011~0.986 | 0.959 |
| Leidenfrost,J(2016) | 0.568 | 0.043~0.975 | 0.874 | |
| Djordjevic,I(2020) | 0.166 | 0.081~0.311 | 0.000 | |
| 合并计算(随机模型) | 0.367 | 0.034~0.905 | 0.704 | |
| 住院病死率 | Riebandt,J(2018) | 0.462 | 0.348~0.580 | 0.530 |
| Luo,XJ(2009) | 0.385 | 0.154~0.682 | 0.456 | |
| Acheampong,B(2016) | 0.340 | 0.195~0.523 | 0.085 | |
| 合并计算(随机模型) | 0.398 | 0.256~0.560 | 0.216 | |
表4 存活率的敏感度分析 |
| 结果 | 文献 | 统计结果 | ||
|---|---|---|---|---|
| 分数 | 95%CI | P值 | ||
| 3个月生存率 | Leidenfrost,J(2016) | 0.711 | 0.595~0.805 | 0.001 |
| den Uil,CA(2018) | 0.796 | 0.670~0.883 | 0.000 | |
| Fischer,Q(2018) | 0.673 | 0.510~0.803 | 0.038 | |
| 合并计算(固定模型) | 0.728 | 0.621~0.814 | 0.000 | |
| 6个月生存率 | Leidenfrost,J(2016) | 0.661 | 0.511~0.784 | 0.036 |
| Fischer,Q(2018) | ||||
| 0.630 | 0.345~0.846 | 0.373 | ||
| 合并计算(固定模型) | 0.654 | 0.522~0.767 | 0.023 | |
| 1年生存率 | Riebandt,J(2018) | 0.626 | 0.364~0.830 | 0.348 |
| Leidenfrost,J(2016) | 0.675 | 0.430~0.851 | 0.157 | |
| Shehab,S(2018) | 0.608 | 0.372~0.802 | 0.371 | |
| Schoenrath,F(2016) | 0.752 | 0.677~0.815 | 0.000 | |
| Han,JJ(2018) | 0.624 | 0.377~0.820 | 0.325 | |
| 合并计算(随机模型) | 0.652 | 0.441~0.817 | 0.154 | |
| 住院生存率 | Taghavi,S(2004) | 0.570 | 0.475~0.660 | 0.147 |
| Bautista-Hernandez,V(2009) | 0.538 | 0.437~0.636 | 0.464 | |
| Luo,XJ(2009) | 0.540 | 0.427~0.650 | 0.485 | |
| Acheampong,B(2016) | 0.579 | 0.479~0.673 | 0.122 | |
| Liu,KS(2009) | 0.545 | 0.449~0.637 | 0.361 | |
| 合并计算(固定模型) | 0.555 | 0.465~0.642 | 0.228 | |
| 总生存率 | Scherer,M(2011) | 0.717 | 0.481~0.874 | 0.070 |
| Chou,NK(2010) | 0.657 | 0.391~0.851 | 0.244 | |
| Scherer,M(2009) | 0.652 | 0.446~0.814 | 0.144 | |
| 合并计算(随机模型) | 0.674 | 0.485~0.820 | 0.071 | |
六、发表偏倚
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
讨论
本研究以系统回顾和荟萃分析,报告了接受ECMO的心功能不全患者的短期病死率和短、中期生存率。包含有18篇高质量文献,一共729例心功能不全患者的观察性研究发现,接受ECMO治疗后的患者长期存活率约为6成。
在1年生存率方面,本荟萃分析一共筛选出5篇文献进行合并,其中,Riebandt等[11]的研究显示,心室辅助装置结合ECMO治疗,可使心功能不全患者的1年生存率为75%。Leidenfrost等[12]研究显示,采用左心室或右心室辅助装置及ECMO治疗的心功能不全患者,其1年生存率为54%。Shehab等[19]的研究显示,采用左心室辅助装置及ECMO治疗的心功能不全患者,其1年生存率为78%。Smedira等[20]的研究显示,单纯ECMO治疗心功能衰竭患者,其1年生存率仅为24%。Schoenrath等[21]的研究显示,因心源性休克产生的心功能不全患者,采用左心室辅助装置或双心室辅助装置,结合ECMO治疗后,其1年生存率为36.8%。Han等[22]的研究显示,采用左心室辅助装置及ECMO治疗的心功能不全患者,其1年生存率为77%。
在住院生存率方面,本荟萃分析一共筛选出5篇文献进行合并,其中,Taghavi等[23]的研究显示,对于心脏移植术后急性右心室衰竭的患者,采用左心室或右心室辅助装置结合ECMO治疗后,其住院生存率为43%。Bautista-Hernandez等[24]的研究显示,采用ECMO治疗先天性心功能不全的儿童患者,其住院生存率为62%。Luo等[14]的研究显示,因心源性休克产生的心功能不全患者,住院生存率落在58%。Acheampong等[15]的研究显示,成人高危先天性心脏病(adult congenital heart disease,ACHD)患者,在接受ECMO治疗后,其住院生存率落在46%。Liu等[25]的研究显示,ECMO治疗先天性心功能不全的患者,其住院生存率为64%。
本荟萃分析存在以下不足:(1)基于医疗伦理方面的原因,ECMO作为心功能不全干预方式的随机对照试验或对照性研究目前很难大范围推广,因此纳入研究数据多为非对照研究,在所有纳入的文献中,病患基线的一致性不确定,可能对结果造成偏差;(2)虽然一共纳入18篇文章,但对于个别研究结局,进行荟萃分析的文章较少,患者数量不足,总体上来说仍缺乏更强有力的临床证据;(3)部分结局异质性较高,虽已按照干预措施的不同,区分出亚组,但由于个别亚组的文献数量不足,无法进一步分析亚组的结果,以克服异质性。
综上,心功能不全患者接受ECMO干预,3个月存活率超过7成,1年存活率超过6成,提示ECMO干预对心功能不全患者有一定的帮助。未来研究须进一步纳入对照性研究,并分析不同的辅助装置是否会对结果产生影响。