
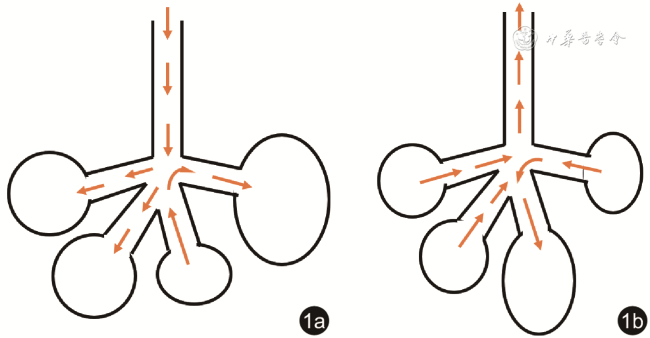
一般认为,对于肺部健康的成年人,呼吸运动是均匀的,各肺泡处于相同的呼吸时相。然而,某些内外科疾病所致的肺损伤,却可能出现局部肺泡通气与整体呼吸运动不协调的情况。在机械通气或自主呼吸的患者中,由于不同病因导致的各肺泡时间常数不同或胸膜腔内压分布不均匀,以致不同肺泡的呼吸时相存在差异,表现为呼吸时气体在肺泡间重新分布的现象,被称为呼吸钟摆(pendelluft)(图1 )。常见的病因包括急性呼吸窘迫综合征(acute respiratory distress syndrome,ARDS)、连枷胸、哮喘和慢性阻塞性肺疾病(chronic obstructive pulmonary disease,COPD)等。随着呼吸监测技术的进步,临床医师和研究者能够更直接地观察和定量评价呼吸钟摆,从而对该现象有更深入的认知。近年来,重症领域学者开始关注呼吸钟摆对重症患者肺部的影响,相关研究方兴未艾。
{kind=link}
{kind=link}
一、呼吸钟摆的理论
“Pendelluft”一词源于德语,在医学文献中出现可追溯至20世纪初,Brauer等[1]用于描述其设想严重气胸的患者呼吸时存在部分气体在两肺间来回摆动的现象。这一词汇被随后的医学研究者沿用。1956年,Otis等[2]首次提出了钟摆现象的理论模型。他们将肺泡的周期性呼吸运动描述为关于时间的正弦函数。正弦函数中的相位,即每个肺泡所处的呼吸时相,受到该肺泡时间常数(顺应性与气道阻力的乘积)的影响。正常情况下,各肺泡所处的呼吸时相一致;当两个相邻肺泡的时间常数存在差异,它们对应的函数相位可能发生偏移,即呼吸时相不一致。在主气道流速归零的吸气末或呼气末状态下,时间常数不一致的相邻肺泡可分别处于吸气相和呼气相,造成气体在肺泡间的交替移动,即为“钟摆”。钟摆现象产生了一个直接结果:即在总体潮气量不变的情况下,发生钟摆的肺泡潮气量将增加,导致局部潮气量之和超过总体潮气量,这也成为了钟摆容积定量分析的基础。2013年,Yoshida等[3]学者基于电阻抗断层成像(electrical impedance tomography,EIT)和胸膜腔内压监测技术,观察到吸气相早期肺内气体由非重力依赖区向重力依赖区转移的现象,将其定义为呼吸钟摆。他们认为,钟摆现象的发生涉及两大要素,一是肺损伤导致的重力依赖区肺泡不张或实变,二是患者存在强烈的自主吸气努力。由于重力依赖区存在肺不张或实变,患者膈肌收缩产生的负压在胸腔内传导不均匀,造成重力依赖区胸膜腔内压更低、跨肺压更大,从而导致肺内部分气体在压力差作用下从非重力依赖区转移至重力依赖区。他们的研究既证实了呼吸钟摆现象的存在,又阐明了自主呼吸和胸膜腔内压差异在呼吸钟摆中的作用,是Otis呼吸钟摆理论模型的重要补充(表1 )。
表1 两种呼吸钟摆理论的对比 |
| 对比内容 | Otis,1956 | Yoshida,2013 |
|---|---|---|
| 理论提出方式 | 数学推演 | 实验印证假设 |
| 钟摆形成条件 | 肺泡时间常数不均 | 背侧肺不张/实变 + 自主呼吸 |
| 自主呼吸 | 不必要 | 必要 |
| 钟摆发生时相 | 吸气末和呼气末期 | 吸气相 |
| 钟摆气体流向 | 吸气末期:时间常数短的肺泡流向时间常数长的肺泡 呼气末期:与吸气相相反 | 吸气相早期:非重力依赖区流向重力依赖区 吸气相后期:与早期相反 |
二、呼吸钟摆的观测
继呼吸钟摆理论模型提出后,研究者尝试利用各种呼吸监测技术证实钟摆现象的存在。Hedenstierna等[4]观察了无肺部疾病的择期腹部手术患者在麻醉状态下的机械通气,应用双腔导管分别描记双肺压力容积曲线。当受试者处于左侧卧位时,通过间断施以呼吸暂停,可记录到两肺容积在短时间内呈相反的变化,提示两肺之间发生了气体移动。Harada等[5]通过置入支气管的若干流速描记仪观察到连枷胸模型实验犬在反常呼吸状态下的气道内钟摆现象。Vyshedskiy等[6]应用多通道呼吸音分析仪记录了90例COPD患者和健康人的呼吸音波形,发现COPD患者在主气道出现呼吸音波形之前往往可记录到小气道呼吸音波形,而在主气道呼吸音波形消失后的一段时间内,仍可记录到小气道呼吸音波形。这种提前出现和滞后消失的小气道呼吸音波形持续时间较健康人显著延长,提示COPD患者存在钟摆现象。2013年,Yoshida等[3]首次通过EIT技术更直观地展示了钟摆现象。EIT可记录肺通气过程的生物电阻抗变化,阻抗变化反映气体的进出。他们观察了机械通气下仍存在强烈自主呼吸的肺损伤患者和实验猪的通气过程,发现吸气时非重力依赖区电阻抗先出现一过性下降而后回升至达峰,重力依赖区电阻抗先上升至达峰而后有所回落,这说明吸气时部分肺内气体先由非重力依赖区向重力依赖区方向流动,随后沿相反方向迁移,即在吸气相出现了钟摆现象。该研究同时应用动态CT技术捕捉到吸气相早期非重力依赖区的气体流失,佐证了EIT的发现。由于EIT技术具有可在床旁、无创、实时监测局部肺通气的优势[7, 8],此后关于钟摆现象的多项研究[9, 10, 11, 12, 13, 14]也借由该技术实现。Tabuchi等[15]首次报道了利用活体暗视野显微镜在直视下观察肺损伤实验鼠模型的钟摆现象。他们在同一视野内识别出吸气相肺泡及其相邻的呼气相肺泡,该现象可发生于整个呼吸周期,而不仅限于吸气末或呼气末期。
三、呼吸钟摆的定量评估
呼吸钟摆现象不仅得到了定性证实,它实际上还是一种可以被定量描述的现象。可以推测,呼吸钟摆的发生频率、范围、容积以及持续时间等参数都有可能影响患者的预后。曾有研究者通过核素示踪剂计算钟摆容积[16],但此类方法显然不适用于临床。Sang等[12]提出一种基于EIT技术定量评估钟摆的方法,他们通过两个维度描述钟摆现象:相位时移(phase shift)和幅度差值(amplitude differences),前者定义为不同肺泡呼吸时相的差异,反映了Otis理论钟摆模型中相位角的偏移程度;后者定义为局部潮气电阻的总和与整体潮气电阻的差值,由于电阻值与潮气量相关性良好,这一差值即反映了钟摆容积,该想法与Otis理论不谋而合。他们分别在2例连枷胸、6例ARDS和COPD急性加重期患者中初步验证了这一算法的有效性:连枷胸患者术后、ARDS患者设置较高水平的呼气末正压(positive end-expiratory pressure,PEEP)或急性哮喘得到控制后,相位时移和幅度差值均减小,而其中1例COPD患者病情进展后,上述两个参数均增加。在另一项用EIT观察了20例自主呼吸试验失败患者的研究中,Coppadoro等[13]也提出了定量计算钟摆容积的方法。他们将整体电阻变化图像沿腹侧向背侧等分为4块感兴趣区(region of interest,ROI),然后根据整体电阻-时间曲线的起伏界定吸气相和呼气相。在吸气相内出现某ROI电阻值下降(提示该区域气体减少)或呼气相内出现某ROI电阻值上升(提示该区域气体增加)即判定为呼吸钟摆。将吸气相与呼气相的钟摆电阻值相加,再通过电阻-潮气量转换系数[17]即可换算为钟摆容积。上述两种基于EIT的方法计算钟摆容积的公式不同,但其原理相近。后者由于并非基于像素点分析,识别钟摆的空间分辨率较低,较前者可能低估钟摆容积。
四、呼吸钟摆的临床意义
在关于高频震荡通气的研究中,钟摆气流被认为是肺内气体交换的重要机制之一[18, 19]。由于高频震荡通气产生的潮气量远小于患者的解剖无效腔,呼吸钟摆有助于肺内气体的混合。但一项生物力学模型分析显示,钟摆现象可使局部肺泡过度膨胀,高速的钟摆气流可增加气道壁剪切应力,可能诱发新的肺损伤[20]。在常规通气中,呼吸钟摆也可能产生类似的后果:由于钟摆现象仅涉及肺内气体重分布,其本身不改变潮气量,这也就意味着对于肺损伤的重症患者而言,即使已经采取了严格的小潮气量通气措施,钟摆仍有可能造成局部肺区潮气量过大[21, 22],成为肺损伤加重的隐性来源。在一项通过生理盐水灌洗和大潮气量诱导实验猪肺损伤模型的研究中[23],实验动物在低PEEP[(6.2±2.4)cmH2O,1 cmH2O=0.098 kPa]和存在自主吸气努力条件下可出现明显的呼吸钟摆和潮式肺复张,呼吸钟摆的幅度与潮式复张肺泡的比例高度相关(Pearson相关系数=0.78,P<0.05)。应用肌松药物后,钟摆现象随之消失,潮式复张肺泡的比例也显著降低[(10.3±1.9)% vs(15.7±6.5)%]。该研究提示钟摆现象可能与自己呼吸所致的肺损伤相关。Morais等[24]在ARDS动物模型中通过正电子发射断层成像技术观察肺内高炎症区域,发现其与EIT在相同动物身上监测的呼吸钟摆区域高度匹配,也说明呼吸钟摆可能加重局部肺损伤。另有研究表明,压力支持通气时存在人机不同步可加重呼吸钟摆[25],表现为发生双重触发前后的钟摆容积均高于正常呼吸的钟摆容积,且双重触发越频繁,钟摆容积可进一步增加,提示呼吸钟摆可能是双重触发导致肺损伤的机制之一。
钟摆现象伴随的局部肺泡过度膨胀和无效通气也可能成为无效腔增加的来源。Coppadoro等[13]根据钟摆容积的多少将20例进行自主呼吸试验的患者分为高钟摆组和低钟摆组,在下调压力支持水平后,2组患者潮气量、呼吸频率和分钟通气量的变化无明显差异,但高钟摆组的钟摆容积变化量[8.8(5.6,12.8)ml vs -0.5(-1.7,1.1)ml]和呼气末二氧化碳分压增加量[3(2,6)mmHg vs 1(0,1)mmHg,1 mmHg=0.133 kPa]较低钟摆组均显著增加,提示呼吸钟摆可伴随通气效率的下降。对于连枷胸而言,有学者认为反常呼吸所致的钟摆现象可能是肺泡通气不足的重要原因,但该观点仍存在争议[5,26]。
重症患者发生肺损伤后,可因低氧、二氧化碳潴留、肺容积减少等机制刺激呼吸中枢,增强呼吸驱动和吸气努力[27]。肺损伤和过强的吸气努力共同作用可诱发呼吸钟摆,而钟摆现象又可以通过降低通气效率使呼吸负荷加重;钟摆现象也可以通过潮式肺复张和局部肺泡过度膨胀加重肺损伤,进一步刺激呼吸中枢,增加呼吸做功,从而增加呼吸钟摆的强度,陷入恶性循环。
五、呼吸钟摆的影响因素及其控制
根据Yoshida钟摆理论,过强的自主呼吸是诱发呼吸钟摆的必要条件,因此也是重要的可干预位点。应用肌松药物可直接降低吸气努力。Yoshida等[3]在肺损伤实验动物模型和1例ARDS患者中均观察到应用肌松药物消除自主呼吸后,钟摆现象随之消失。此时不同肺泡区域虽然充气和放气的速率有所不同,但呼吸时相保持一致。相似地,Pellegrini等[28]对轻度ARDS实验猪应用肌松剂消除自主呼吸后,也观察到吸气相早期由非重力依赖区流向重力依赖区的钟摆现象随之消失。但不同的是,在完全控制通气的整个吸气相内,他们通过动态CT仍可观察到肺内气体的重分布现象(gas displacing and gas scattering),这种钟摆的方向在解剖上没有规律,它有可能是由于相邻肺泡时间常数不同而发生的。肌松药物虽然可以很好地控制Yoshida钟摆,但它的使用也存在需要深镇静、延长镇静时间、增加ICU获得性衰弱的风险等副作用[29],甚至抵消它的益处,在中重度ARDS的随机对照试验中呈现阴性结果[30]。近年的研究也提示吸气努力过低或过高均不利于膈肌保护[31, 32, 33],需要在控制有害钟摆和避免膈肌萎缩之间寻找平衡点,而采用“部分肌松”策略定量控制吸气努力可能是一种解决方法[34]。
在Otis和Yoshida钟摆理论中,诱发呼吸钟摆的共同要素是存在肺泡异质性,这也是可干预位点。有生理学研究提示肺泡异质性越大,钟摆效应越显著[35]。因此,控制钟摆也可从这方面着手。ARDS患者可存在显著的肺泡异质性,设置合适的PEEP有助于改善肺泡异质性[36]。Morais等[24]观察了PEEP对存在强烈自主呼吸的ARDS实验动物和患者的影响。相比于较低的PEEP(5~8 cmH2O),使用高PEEP(13~15 cmH2O)一方面降低了食管压的呼吸变异程度,即降低吸气努力,另一方面使得重力依赖区和非重力依赖区的胸膜腔内压分布更均匀。伴随的结果有呼吸钟摆相关潮式肺复张和重力依赖区过度膨胀的减轻,以及组织学结果提示肺损伤程度较轻。该研究也提示合适的PEEP可能有助于减少或避免肌松药物在中重度ARDS患者中的使用。相比于改变PEEP,调整其他呼吸机参数,如吸气触发灵敏度、压力上升时间、压力控制模式下的吸气时间,或比较压力控制和容量控制模式,对呼吸钟摆的影响甚微[37]。另有研究表明,在容量控制模式下提高吸气流速,肺泡异质性增加,钟摆容积也增大[38]。俯卧位也是促进肺复张、改善ARDS患者肺泡异质性的重要措施[39],然而其对呼吸钟摆的影响仍有待被研究。
六、呼吸钟摆的研究方向
综上,部分肺损伤的重症患者可发生呼吸钟摆,即肺内气体重分布的现象。过强的自主吸气努力是呼吸钟摆的重要诱因。该现象发生隐匿,但可通过导致潮式肺复张、局部过度膨胀和通气效率下降等机制,进一步加重肺损伤,需要重症医师提高警惕。EIT技术是目前临床观察重症患者呼吸钟摆现象的最佳选择,它能够定量描述钟摆强度。未来需要明确钟摆强度和临床预后的关联,以指导医师对该现象的合理干预。