
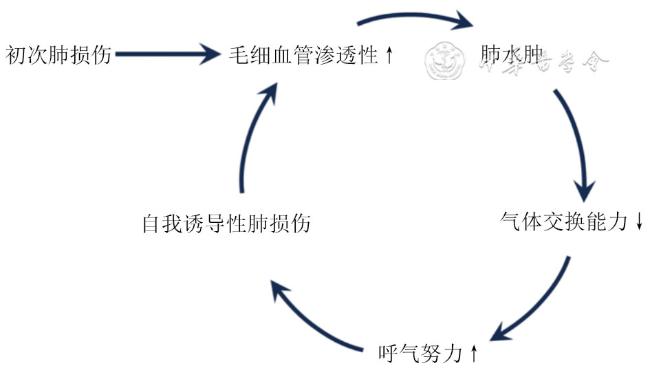
急性呼吸窘迫综合征(acute respiratory distress syndrome,ARDS)是临床常见的重症疾病,全球ICU中约有10%的患者患有ARDS,中重度ARDS患者病死率高达40%以上,过去3年间新型冠状病毒感染的大流行更是导致ARDS发病率大幅上升[1-2]。ARDS的突出病理生理变化在于肺泡塌陷带来的肺容积减少,刺激气道平滑肌中的肺牵张感受器,通过迷走神经传入呼吸中枢触发肺牵张反射;随之经运动神经传出一定强度的呼吸驱动引发膈肌动作电位,最终表现为膈肌收缩。此外,中枢及外周化学感受器对动脉血气和pH变化的反应、神经内分泌反应,均是呼吸驱动力的重要决定因素。然而,ARDS患者呼吸驱动的增强则造成过强的吸气努力,可能加重呼吸窘迫症状,表现为过度的全肺及局部应力、肺水肿加重、肺内气体摆动等,最终导致自我诱导性肺损伤(patient self-inflicted lung injury,P-SILI)(图1)。此外,过强的呼吸驱动使得机械通气治疗面临挑战,常导致患者出现人机不同步,进一步引发相关性膈肌功能障碍。
{kind=link}
{kind=link}
针对高呼吸驱动患者,临床治疗中有多种干预手段。经鼻高流量氧疗及无创正压通气通过改善肺通气及顺应性可有效降低驱动压[3],机械通气治疗中较高的呼气末正压(positive end-expiratory pressure,PEEP)设定也可降低吸气努力。此外,俯卧位通气、体外CO2清除也可有效改善患者呼吸驱动。若应用以上方法未见明显成效,在充分镇痛镇静的基础上,中重度ARDS仍存在过强的呼吸驱动时,可加用肌松剂,从而预防自主呼吸过强可能导致的肺与膈肌损伤。
肌松剂即神经肌肉阻滞药物(neuromuscular blocking agent,NMBA),可以阻断神经肌肉接头的信号传导,诱导神经肌肉阻滞,从而控制机械通气治疗中患者的自主呼吸,避免进一步肺损伤及膈肌功能障碍。然而,循证医学证据表明,早期使用肌松剂对中重度ARDS患者病死率的降低效果并不显著[4-5]。由于既往肌松程度监测技术的限制及监测意识的淡薄,ARDS治疗中肌松剂滥用的现象时有发生,这也导致多种并发症及预后的恶化[6],最新欧洲重症医学学会(European Society of Intensive Care Medicine, ESICM)指南明确指出,在ARDS治疗中不推荐常规使用肌松剂用于降低病死率[7]。然而,临床对待肌松剂的使用在保持警惕的同时,并不能因其滥用所致的危害而因噎废食。针对过强自主呼吸驱动病因,有着多种干预治疗手段,包括加强镇静镇痛、合理呼吸机辅助、CO2清除及俯卧位通气等等。因此针对有肌松剂使用指征的患者进行肌松剂量的滴定,从而选择个体化肌松方案是ARDS临床治疗的重要环节[8]。为进一步优化肌松治疗的个体化实施,本文对ARDS患者肌松滴定的研究进展进行综述,旨在为ARDS患者临床治疗选择合适的肌松深度提供依据。
一、肌松滴定的必要性:深度适可而止
(一)肌松过浅难以规避损伤:不尽如人意
(二)过度肌松引发系列问题:弊大于利
(三)选择最佳肌松剂量:趋利避害
二、如何评价肌松效果实现肌松滴定
针对ARDS的治疗往往牵涉多方面的复杂因素,由于患者存在个体化差异性,给予相同剂量的肌松药物,不同患者可能表现出各不相同的阻滞水平[19]。临床中运用侵入性及非侵入性的多种手段监测自主呼吸触发以评价肌松效果,是实现个体化肌松滴定的重要组成部分,也是ARDS个体化精准治疗的重要部分。
(一)侵入性
1. 食管压(esophageal pressure,Pes)摆动:Pes通过球囊技术反映胸腔内压,其在自主呼吸过程中产生的摆动(△Pes)是反映ARDS患者肌松深度的有效指标。△Pes在3~15 cmH2O(1 cmH2O=0.098 kPa)时接近生理范围,可作为肌松滴定的目标[20]。一般来说,吸气努力可以由呼吸肌的压力-时间乘积(pressure-time product,PTP)来量化,Vaporidi等[21]的研究验证了Pes在吸气末和呼气末的差值与PTP的相关性,因其比PTP易于床旁获取,是吸气努力更为简单易得的替代指标。△Pes>7 cmH2O表明患者存在呼吸努力,△Pes>14 cmH2O可用于识别存在极强吸气努力的患者。此外△Pes还可以用于监测患者-呼吸机的不同步现象。然而由于Pes是对胸膜压的间接估计,准确性受到导管插入技术、球囊定位等影响,因此临床的应用与推广受到一定局限。
2.膈肌电活动(diaphragm electrical activity,EAdi):EAdi即在远端配备微型电极的专用鼻胃饲管监测到的膈肌电活动,是临床实践中可用的“最接近”的神经呼吸驱动替代,可应用于临床肌松滴定。Liu等[22]发现EAdi的峰值和基础值反映患者呼吸肌电活动的强弱,主要反映中枢神经驱动对膈肌的兴奋。Mauri等[23]的研究验证EAdi和△Pes在不同呼吸支持水平上均呈现一致的摆动。与呼吸机波形(例如流量和气道压力)一起,EAdi同样可用于识别患者-呼吸机相互作用。然而由于患者个体差异大(年轻健康受试者为4~29 μV),因此没有明确的EAdi生理参考值。可见,EAdi可作为一种趋势指标来监测同一患者,在肌松滴定中具有准确、高效等诸多优势。
(二)非侵入性
1. 四个成串刺激(train-of-four,TOF):TOF即通过监测肌肉松弛程度量化肌松深度的监测技术,对临床肌松滴定有指导价值。在外周运动神经上施加4次连续的刺激(频率通常为2 Hz),并测量相应肌肉的收缩反应,这4次刺激产生的肌肉收缩通常被表示为T1、T2、T3和T4。神经肌肉兴奋传递正常的情况下四个成串刺激比值(train-of-four ratio,TOFr)即T4/T1接近于1。一项针对ARDS患者的前瞻性研究表明,根据TOF监测目标(T2/T4)管理肌松药物的使用,可以有效降低肌松药物损耗,同时不影响神经肌肉阻滞的预期[24]。Thompson等[25]的研究也表明,使用TOF监测滴定肌松后肌松效果虽无明显差异而用量缩减3倍,有效降低了液体超负荷的风险。然而TOFr与患者氧合水平相关性低,作为监测指标略显单一,同时存在操作人员主观差异大及电极传导不良等局限[26]。在实际操作中,TOF监测须结合患者的临床指标,才能实现更为准确全面的肌松滴定。
2. 膈肌超声:超声通过监测自主呼吸所产生的膈肌变化反映肌松深度,是无创、可重复的床旁肌松滴定手段[27]。超声评估重点在于膈肌运动幅度变化及膈肌厚度变化[28],即膈肌偏倚(diaphragm excursion,DE)与膈肌增厚分数(diaphragm thickening fraction,DTF)。膈肌偏倚差(diaphragm excursion difference,DED)即深呼吸与安静呼吸状态下DE的差值,Lang等[29]的研究表明DED与TOFr呈正相关,并具有高度特异性[30]。膈肌的超声评估为反映吸气努力提供重要信息,然而目前基于DED与DTF判断膈肌肌松尚未有明确截断值,临床应用超声滴定肌松仍有待进一步研究。
3.压力肌肉指数(pressure muscle index,PMI):PMI通过呈现呼吸肌所产生的压力可以准确反映肌松深度。PMI是基于呼气末阻塞试验(end-expiratory occlusion test,EEOT)测得的由呼吸努力产生的呼气末气道压力差值,即吸气末闭塞的Pplat与呼吸机施加的压力[PEEP+压力支持通气(pressure support ventilation,PSV)]之间的差值[31]。通过该方法表征自主呼吸程度,不仅可以反映患者吸气努力,也可以识别各种人机不同步现象。然而PMI需要间歇吸气屏气或复杂的计算,且阻塞期间没有呼吸努力并不能排除反向触发导致的呼吸努力[32]。因此临床需要更为简单易得的监测指标指导肌松药物的滴定。
三、临床优化机械通气策略:肺与膈肌保护性通气
(一)避免盲目肌松带来的损害
(二)实现肺与膈肌保护性通气
机械通气是ARDS患者治疗的挽救性措施,但往往导致肺的二次损伤与膈肌损伤或萎缩。既往研究表明,预防P-SILI需要适当的肌松深度,以消除或减少呼吸努力的强度;此外,机械通气本身会使膈肌发生明显的急性结构改变,引发膈肌功能障碍[13]。选择恰当的肌松水平,有助于维持合理的呼吸驱动,从而降低呼吸机相关性肺与膈肌损伤,帮助实现肺与膈肌保护性通气。肺与膈肌保护性通气是保护性机械通气的重要组成部分,有助于患者肺与膈肌功能的保留,对机械通气患者早日脱机具有重要意义。
四、小结
肌松治疗对ARDS机械通气患者实现膈肌保护性通气具有重要意义。在ARDS临床治疗中,应当谨慎选择适合不同患者的肌松水平。目前可通过无创及有创等多种手段进行肌松深度的监测,实现肌松水平的合理滴定,是避免肺与膈肌损伤的安全保障。但肌松床旁滴定仍缺乏确切可靠的金标准,有待进一步临床研究。